Biology concepts – evolution, reproductive advantage, natural selection, co-dominance, X-linked genes
Last week we learned how less aggressive strains of malaria were used to treat neurosyphilis and how they may be useful in treating HIV infection. This week, we will turn 180˚ and see if other diseases can help prevent or lessen the effects of malaria. In the process, much can be learned about natural selection and reproductive advantage.
 |
Plasmodium-infected red blood cells develop knobs, the surface protrusions seen on the left erythrocyte. These knobs are covered in a certain protein that inhibits the immune system’s ability to recognize this cell as infected and respond to it. The cell on the right is also infected with P. falciparum, but has a mutation that prevents knob formation. Image credit: Ross Waller and Alan Cowman. |
As youundoubtedly remember from last week, malaria is a parasite-caused infectious disease that is transmitted from human to human by mosquitoes. The parasite, Plasmodium falciparum, takes up residence in the red blood cells (RBC) to reproduce. The red cells burst to release the organisms, and this brings fever and weakness.
As far back as the 15th and 16thcenturies, quinine, made from the bark of the cinchona tree, was being used in Peru to treat malaria. Chloroquine, mefloquine, and quinine all work against malaria in similar fashion. Because of their neutral pH, they move across membranes easily including the lysosomemembrane. Once inside the lysosome, they become charged and can’t get out. This includes the trophozoite-containing lysosomes. In the RBC, trophozoites consume hemoglobin to obtain amino acids, and the heme is digested in the lysosomes to form a black malaria pigment. The quinine drugs in the lysosome bind up the heme and produce a toxic product (cytotoxic heme) that kills the parasite.
There are other classes of drugs that are useful against P. falciparum. Primaquine and the artemisinin drug, artesunate, act by a completely different mechanism from that the quinine drugs. Artesunate is excellent for treating P. falciparum malaria, while primaquine is often used in conjunction with quinine to treat P. vivax or P. ovale forms of the disease.
These drugs work by breaking down – weird, but this is how many drugs work. It isn’t what you swallow that kills the organism, it's the metabolites (the products made by your biochemistry breaking down the drug) that are active. In the case of artesunate and primaquine, the heme molecule in the red blood cells releases peroxide from the parent compound (the drug you take). This is just like the peroxide you use to wipe out cut in order to prevent infection.
 |
Artusenate comes from the sweet wormwood plant. Chinese herbal medicine has used it for thousands of years. A recipe for an Artemisia based malaria medicine was found on a tablet from the Han Dynasty (206 BCE to 20 CE). It is now being investigated as a treatment for breast cancer, also based on its ability to form radicals. |
The cell has defenses against free radical damage, but higher than normal concentrations render the RBC fragile; on the tipping point of destruction. Treatment with primaquine or artesunate makes the cell inhospitable for the parasite, the red blood cells become flop houses instead of five star hotels. The parasite’s operating instructions are to survive and reproduce, but these drugs pull up the erythrocyte welcome mat and the parasite seeks moves on to seek friendlier accommodations.
Unfortunately, some strains of P. falciparum have become resistant to some quinine drugs, especially chloroquine. The free radical generating drugs are still useful, but scientists in Western Cambodia recently reported artesunate drug resistance there. The parasite has evolved – evolutionary pressure is everywhere. The actions of humans have put pressure on the organism to evolve; those parasites with mutations to resist the drugs have a reproductive advantage, and those mutations get passed on. We had better have something else on our plate to combat malaria – we're working on it, but nature has provided some help as well.
There are natural defenses against malaria. We have seen that a fragile red blood cell helps in preventing are lessening the disease course of malaria. What else might do that? This is where human genes come into play.
Sickle cell diseasecreates a very fragile RBC. The mutation is just a single DNA base change in the hemoglobin beta chain peptide, but the result is a hemoglobin molecule that becomes pointy and can tear the red blood cell apart, or can get stuck in small blood vessels and prevent good blood flow. Reduced blood flow starves the downstream tissues of oxygen.
You get one gene for hemoglobin beta chain from each parent. The disease comes when an individual receives mutated genes from both parents. But that doesn’t mean that sickle cell anemia is a recessive trait. If you have one copy of the mutated gene, then you will have sickling problems when oxygen concentrations are low, like during exercise or at high altitude.
 |
Sickle cell disease or a sickle cell trait episode can result in red blood cells clogging up vessels and organs. On the left is an absolutely HUGE spleen from a sickle cell patient. On the right is a normal sized spleen, about 20% the size of the injured spleen on the left. A normal spleen is about the size of your hand, maybe a little skinnier. |
If sickle cell anemia was a recessive disease, then a single wild type (normal) gene would be dominant, and you would show no disease. Instead, sickle cell anemia is co-dominant, one mutated allele (copy of the gene) is like having half the disease; it only shows up in certain circumstances.
This can still be a pebble in your shoe, just ask Ryan Clark, the Pro-Bowl safety for the Pittsburgh Steelers. In a 2007 game in Denver (altitude 5300 ft, 1616 m), Ryan almost died from a sickling attack during the game, and ended up having his spleen and gall bladder removed (remember that sickled RBCs can clog blood vessels, especially in blood rich organs like the spleen).
When Pittsburgh next played Denver, Clark didn’t even make the trip. This just happened to be the 2011 playoff game in which Tim Tebow threw a long touchdown pass in overtime to the receiver being covered by Clark’s replacement. Sometimes disease can change how sports evolve as well.
Thalassemia is another example. This is a group of inherited disorders wherein there is reduced production of one of the subunits of hemoglobin (hemoglobin is made from 2 alpha and 2 beta subunits). Alpha-thalassemias have mutations in the alpha subunit; likewise for beta-thalassemia.
Reduced subunit number means reduced hemoglobin number; the blood won’t carry enough oxygen, and the patient is constantly oxygen-poor in his/her tissues. Having two mutated alpha genes is lethal in the very young (called hydrops fetalis), but you can live with one mutated alpha gene, one mutated beta gene, or even two mutated beta genes.
 |
This the broad bean, or fava bean in opened pod and out of the pod in a bowl. The ancient Greeks used to vote with fava beans, a young white bean meant yes, and old black one meant no. |
Favism, better called glucose-6 phosphate dehydrogenase deficiency (G6PDH), is an X-linked genetic disease; the gene is on the X chromosome. A female (XX) has two copies, so having one mutant copy is no problem, but a male (XY) has only one, so getting a mutated copy from your mother means that you ONLY have the mutated gene – this brings the disease.
The enzyme G6PDH works in several pathways; in your red blood cells, it is the only source of reduced glutathione, an important antioxidant. This means that things that trigger free radical formation in your red blood cells will trigger the disease – lots of weakness and lack of energy. If there is enough erythrocyte destruction, one could die.
Triggers include broad beans (fava beans), hence the name favism. Other triggers include many drugs, including primaquine and artesunate, the anti-malaria drugs that induce free radicals. Having G6PDH-deficiency is like having your own artesunate pharmacy right in your cells - you naturally have higher oxygen radical levels in your RBCs, so the malarial parasite can't live there.
Not by accident, sickle cell mutation is more prevalent in people of Sub-Saharan African descent, thalassemia mutation is more common in people from the warm, moist Mediterranean, and G6PDH-deficiency is found most commonly in the Mediterranean and Southeast Asia. These just happen to be the areas where malaria-carrying mosquitoes are most abundant. Evolutionary biologists make the argument that natural selection has maintained these genes in the populations because they provide a reproductive advantage to the species.
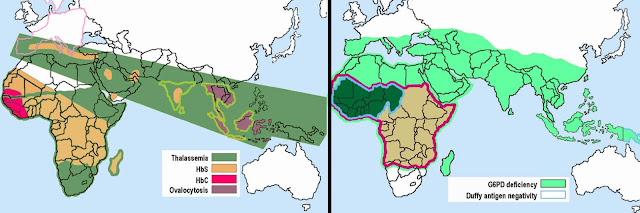 |
Left image: dark green is where there is thalassemia and yellow and red are where there is sickle cell. Right image, light green is where there is favism, and inside the light blue outline is duffy antigen mutation. It is interesting that these areas are also where malaria is endemic. |
Youmight die from sickle cell disease, but probably not from sickle cell trait or beta-thalassemia. Learning not to eat fava beans makes the G6PDH mutation less lethal. One might very well live to an age where one could mate and pass on his/her genes. The diseases might still kill the patient, just not as soon as malaria would.
Malaria is a killer, and significantly, a killer of the young. In East Africa, children are bitten by the anopheles mosquito on average 50-80 times each month. They very well might not reach an age to reproduce. Therefore, having sickle cell trait, thalassemia, or favism provides a reproductive advantage in these environments and natural selection has resulted in these alleles remaining in the populations in these areas.
 |
The Duffy antigen (DARC) is important for P. vivax entrance into the red blood cell. The Duffy binding protein (DBP) interacts with DARC, the yellow parts of the DBP are variable, and can be used to bind an antibody. These variable areas overlap the binding site, and can be used to make a vaccine for P. vivax. |
SinceP. vivax uses Duffy Ag as a way to enter the red blood cells, those with the Duffy SNP are resistant to P. vivax malaria – they don’t even have to suffer with some other disease; just a simple case of chance. And the prepared mind exploits chance – the Duffy antigen binding protein is now a candidate for use as a P. vivax vaccine.
Next week, how the plague was defeated by a genetic disease.
Chootong P, Panichakul T, Permmongkol C, Barnes SJ, Udomsangpetch R, et al. (2012). Characterization of Inhibitory Anti-Duffy Binding Protein II Immunity: Approach to Plasmodium vivax Vaccine Development in Thailand. PLoS ONE , 7 (4) DOI: 10.1371/journal.pone.0035769
For more information or classroom activities, see:
Malaria –
sickle cell mutation –
thalassemia –
favism –
duffy antigen –