Biology concepts – lipids, fatty acid, saturated fat, trans fat, interesterification, adipose tissue, lipodystrophy, LDL and HDL
Most of us worry about gaining weight. We would love to be skinnier, lighter, trimmer, svelter (a new word?). But what if you had the opposite problem – you couldn’t gain any weight, no matter how much you ate?
A 2013 study sought to determine why the opposite things happen with fat in different places. They tracked different markers in each location and found that mitochondrial changes were the same in visceral adipose tissue (VAT) and subdermal adipose tissue (SAT). But the signals to build fat decreased only in SAT. Most telling, inflammatory signals were much greater in SAT than in VAT; it may be that less inflammation leads to less fat wasting. Strange that fat would be linked to inflammation – or maybe not - keep reading.
Glucose first gets stored as glycogen, but we make only a certain amount of glycogen. Usually a human has about one lazy day’s worth of glycogen. Energy beyond that gets stored as fat, and that’s a good thing. Imagine how large we would all be if we all our energy reserves were in the form of glycogen + water. A normal human adult male would weigh an extra 110 pounds (50 kg)!
However, saturated fats are good at promoting liver and lung health, so some saturated fat in your diet is not a bad thing. Trans-fats, on the other hand, are harder to discuss. They can be made in a factory by removing some double bonds from polyunsaturated fats by partial hydrogenation. They also occur naturally, but are very rare compared to cis fats, so they don’t usually cause a problem.
When you eat saturated fats, both the LDL and the HDL levels increase, so the ratio stays generally the same. With trans-fats, the LDL production goes up but the HDL level stays the same or decreases. This leads to a bad ratio and disease progression.
By stealing the cholesterol from LDL, HDLs also stop many mechanisms that can lead to vessel blocking, like the stimulation of vessel inflammation by LDLs, the formation of clots in the vessels (HDLs are anti-thrombotic, a thrombus is a clot), and by preventing the oxidation of LDLs.
Gallego-Escuredo JM, Villarroya J, Domingo P, Targarona EM, Alegre M, Domingo JC, Villarroya F, & Giralt M (2013). Differentially Altered Molecular Signature of Visceral Adipose Tissue in HIV-1-Associated Lipodystrophy. Journal of acquired immune deficiency syndromes (1999), 64 (2), 142-8 PMID: 23714743
Xu S, Liu Z, & Liu P (2013). HDL cholesterol in cardiovascular diseases: The good, the bad, and the ugly? International journal of cardiology, 168 (4), 3157-9 PMID: 23962777
Barter, P. (2005). The role of HDL-cholesterol in preventing atherosclerotic disease. , 7(Suppl F), F4-F8. European heart Journal, 7 DOI: 10.1093/eurheartj/sui036
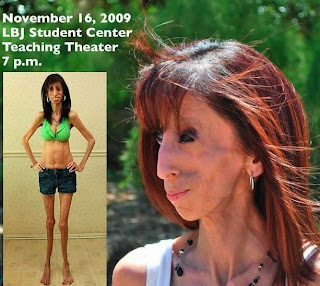 |
This is Lizzie Velasquez, a 24 year old with a genetic form of lipodystrophy. She must consume 5000- 8000 calories and eat 80 times each day just to survive. Her condition is called neonatal progeroid syndrome, which includes premature aging and an oversized head along with the lipodystrophy. She has dealt with more than any person should have to, and now is a motivational speaker – "it’s going to get better" is her theme. Her second book, Be Beautiful, Be Youis a must read. The picture is from one of her public talks. |
There is a group of disorders known as the lipodystrophies (lipo = fat, dys = bad, and trophy = nourishment) in which afflicted people can't store any fat. Their stories tell us that being skinny is no blessing.
Lipodystrophies can be congenital(con = with, genitus = to beget), so they are present from conception, or they can be acquired. In congenital cases, the genetic mutation sometimes has little to do with fat, sometimes it does. There are four known mutations in four different proteins that can all lead to a lipodystrophy.
People with a congenital lipodystrophy tend to develop type II diabetes. They also get arthritis and other disorders. Some mutations also carry higher risks of mental retardation and most increase the risk of cardiac disease and cirrhosis of the liver. These can kill you.
Acquired forms often result from drug treatment. In HIV retroviral treatment, there can by lipodystrophy and lipoatrophy– which is loss of fat from one particular anatomic location, usually the face. On the other hand, visceral fat (fat around the internal organs) is increased during anti-HIV treatment. It matters, since visceral fat is associated with more heart and liver disease.
 |
Lipoatrophy refers to the loss of fat in a particular area of the body. On the left is the facial atrophy seen in patients on anti- viral therapy in HIV infection. On the right is a specific lipoatrophy surrounding an insulin injection sight for diabetes. |
Fat may be considered evil, but it serves a purpose. The problems that lipodystrophy patients encounter underline that fat is a necessary tissue for animals. Problems arise when you accumulate too much of it, either under your skin, around your organs, or in your blood. If you don’t use the calories you take in for energy, your body will store them for later.
Chemically, a fat is made up of three fatty acids (see below)attached to a 3-carbon glycerol molecule. In adipose tissue (from latin aipem = fat) and subcutaneous fat, these triglycerides, also called triacylglycerols (tri = 3, glycer = glycerol, and acyl = acid) are stored until they are released to the blood stream as fatty acids alone. The fatty acids can then be broken down and used to generate ATP in the cells.
Fats are a much more efficient storage form of energy as compared to glucose or glycogen. There is 4.5 x more energy in fat as compared to the same mass of glycogen or glucose. In addition, since fats are hydrophobic (hydro = water, and phobic = fearing), they can be stored without water. These two factors mean that a lot of energy can be stored in a little space.
A fat molecule is really a triglyceride. The right structure is a typical triglyceride with three fatty acids in black connected to the bluish glycerol. By ester bonds in dark red. A trans double bond is shown in green. On the right is the partial hydrogenation process that converts a polyunsaturated fat into a trans fat. Usually there is a mix of products, with some cis bonds being converted to trans bonds. |
A fatty acid is a chain of carbons with a carboxyl group (HO-C=O) on one end. If the chain of carbons contains only single bonds, then the fatty acid is called saturated. If there is one double bond between carbons, then it is an unsaturated fatty acid, and if there are two or more double bonds (unsaturations), then it is a polyunsaturatedfatty acid.
The same terminology is used for triglycerides (fats) made from the fatty acids. A fat with only saturated fatty acids is a saturated fat. The double bond type also makes a difference for the fatty acid and fat. If the bond is in one configuration, it is called cis, and it creates a bend in the chain. If the double bond is in the other configuration, then it is called trans, and it is much straighter, like a saturated fatty acid.
You have heard of the benefits of polyunsaturated fats as opposed to saturated fats, and of the evils of trans-fats. Saturated fats tend to produce bad results in the blood stream. Their breakdown results in more acetates which stimulate cholesterol production. Also, saturated fats tend to clump together and form blockages in vessels. This leads to atherosclerosis and can kill you.
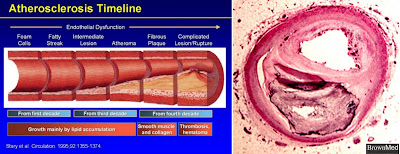 |
The left cartoon shows the buildup of plaque over time in atherosclerosis. It takes along time, but we all seem to be working hard to make it happen. The right image is a photomicrograph showing the blockage in a large coronary artery. Think the amount of blood getting through is enough to nourish your heart? Think it’s going to have a happy ending? |
The vast majority of trans fats we eat are industrially made. The trans double bonds are created in the hydrogenation process (adding hydrogens to reduce the number of double bonds). Some cis- double bonds become trans- double bonds during the process.
Industry likes the saturated and trans-fats because they tend to be more solid at room temperature (higher melting temperatures). Saturated and trans-fats have more hydrogens (see picture above). The kink in trans-fats also increases the melting temperature.
The hydrogens and kinks lead to more interactions between the different molecules – they hold on to one another more tightly. Melting is basically making the different molecules separate by adding energy, so the added hydrogens have the end result of raising the melting temperature. This is good for making things like margarine.
Unfortunately, trans-fats tend to increase low-density lipoprotein (LDL) production; these contribute greatly to artery clogging and heart disease. The blocking of arteries is bad enough, but if they occur in the brain, or if part of a plaque breaks off, travels to the brain and blocks a vessel – that’s a stroke. There’s not much that’s worse than a stroke.
Saturated fats also raise the levels of LDL’s - so why are trans-fats worse for you than saturated fats? The levels of LDLs are only one aspect in disease promotion, the level of the good-for-you HDLs (high density lipoproteins) is just as important. It's the ratio of LDL:HDL that matters.
 |
In the space of the vessel are some large cells with very light cytoplasm that looks like Swiss cheese. There are many small clear droplets and some larger ones. These are fat droplets and give the cells their name – foam cells. You can see that some have more than one nucleus. Two diseased macrophages will often merge into multinucleate giant cells. |
The next question then is how do HDLs help prevent disease caused by LDLs? LDLs supply cholesterol to the cells that need it – and that’s all your cells (more on this next week). But if there is too much LDL, then they start to accumulate in the vessels and can form things like foam cells.
Foam cells are tissue macrophages located in/on the vessel walls. The job of macrophages is to eat things, so these macrophages eat up the extra LDLs in the area - but they don’t break them down. They build up and start to look like foam inside the cell. Unfortunately, the macrophages then become part of the problem; as they accumulate they form fat streaks in the vessel wall. This is the beginning of plaque formation and atherosclerosis.
A 2005 review looked at how HDLs are health promoting. It turns out that they steal cholesterol from LDLs, but they don’t promote the formation of foam cells and plaques because of their different structure. Therefore, having more HDLs will rescue more cholesterol from LDLs and transport it to the liver for eventual destruction.
 |
The top cartoon shows how HDL help get rid cholesterol after it has been phagocytosed by a macrophage foam cell. A pre-HDL interacts with receptors on the macrophage which then transfer cholesterol to the HDL. This is taken to the liver where it is broken down and reused for bile production. This is called reverse cholesterol transport. The bottom image shows the functions of HDL, even beyond its ability to negate the unhealthy effects of LDLs. |
Oxidation of LDLs leads to oxygen radicals can damage vessel cells and promote plaque formation. But HDL complexes include an enzyme called paraoxonase, which prevents the oxidation of closely associated LDL molecules. Preventing oxidation also reduced the production of pro-inflammatory molecules in the vessel wall and decreased the recruitment of some inflammatory cell to the area. Hurrah for HDL!
But wait – of course there’s an exception. HDLs from patients with existing diseases, like coronary artery disease (CAD) or chronic kidney dysfunction (CKD) actually contributeto plaque formation rather than prevent it! A 2013 review talked about how HDLs from CAD patients limit the anti-inflammatory and repair processes in the vessels cells, and in CKD patients promote inflammation and raise blood pressure. I guess the best way to prevent atherosclerosis is to not develop atherosclerosis.
Overall, you want to reduce fat intake, but especially trans-fats and saturated fats. Food labels are now required to show how much trans fat is in the product, but the manufacturers are getting around the regulation. They combine different fatty acids in a fat and they call them interestrified fats. Partial hydrogenation is still a major factor, but they aren’t called trans-fats. This allows them to keep it below the FDA radar. Interesterified fats don’t exist in nature – that should tell us all we need to know.
What we need is a way to partially hydrogenate the polyunsaturated fats that does not create trans-fats – you work on that while I butter my bagel. Next week we can look at more aspects of fats, and how they are different from the other lipids.
For more information or classroom activities, see:
Trans fats –
interesterification –
LDL:HDL –
http://www.medindia.net/news/reverse-cholesterol-transport-a-cholesterol-removal-system-116495-1.htm